[Update: On 30 Nov, Moderna announced its Primary Efficacy Analysis, with updated results from its clinical trial, further validating its efficacy, particularly against severe Covid-19 symptoms. However, the key points in my article still stand while we await the full results, which would include data on whether the vaccine prevents asymptomatic infections.
What was new in this announcement was Moderna’s statement that “Efficacy was consistent across age, race and ethnicity, and gender demographics.” I would love to see this breakdown, which was unfortunately not included in here.]
With announcements of being ~95% “effective”, the Moderna and Pfizer vaccines are being viewed as magic bullet(s) to end the havoc wrecked by Covid over this past year. But are they really?
Over this year, I have learnt that confirmation bias and attention-grabbing news headlines make for a dangerous cocktail. As humans, we see what we want to see. For one, for those of us who saw the 95% figure and assumed it would definitively reduce Covid infection—here’s one less well-publicized caveat from Moderna’s chief medical officer in an Axios interview:
They [clinical trial results] do not show that they prevent you from potentially carrying this virus transiently and infecting others.” — Tal Zaks, Moderna Chief Medical Officer
In other words, the 95% figure was calculated based on trial participants who developed Covid symptoms. Would we get the same results if Moderna/Pfizer had run Covid tests on all the participants? Would this figure change if we look at high-risk groups?
In this article, I embark on my personal journey of curbing my ignorance towards vaccines as I dig further into the touted 95% figure and its implications.
TL;DR —Based on the trial results, the vaccines are a triumph of science in preventing the general population from getting severely sick. What I am cautiously optimistic towards is concluding too early that the vaccine will end Covid, given the absence of evidence in the case of asymptomatic infections and its efficacy on specific high-risk groups such as the elderly. Not to mention the logistical and trust hurdles present in vaccine distribution.
A fitting quote from a credible source himself:
“Absent proof, I think it’s important we don’t change behavior solely on the basis of vaccination.” — Tal Zaks, Moderna Chief Medical Officer

Given that my ability to Google most probably outweighs any expertise I have on Covid and on vaccines, I have cobbled together some views based on what I have been able to gather from credible sources. Here, pardon my bias towards focusing largely on Moderna, since they were the first to get to that 95% efficacy/effectiveness figure after all.
Questions I explore:
- Does the 95% figure mean that once vaccinated, I only have a 5% chance of getting sick with Covid?
- Does the 95% effectiveness rate generalize to me, if I am a high-risk individual above the age of 65?
- With a 95% effectiveness, does this mean that Covid transmission will be halted in its tracks?
- Once I get vaccinated, does this mean I can go out and live life as it was pre-Covid?
Question #1: Does the 95% figure mean that once vaccinated, I only have a 5% chance of getting sick with Covid?
It’s more complicated than that. First, it is important to understand how 95% is calculated. Let’s look at Moderna’s figures:
This first interim analysis was based on 95 cases, of which 90 cases of COVID-19 were observed in the placebo group versus 5 cases observed in the mRNA-1273 group, resulting in a point estimate of vaccine efficacy of 94.5% — Moderna, Nov 16 press release

The diagram above shows that the number of actual Covid cases identified makes up a very small fraction of the overall participant pool.
For those new to the science of vaccines (including myself): let’s be clear here, Moderna did not expose all 30,000 participants to Covid (very bad idea!) before concluding that only 94.5% of them ended up getting Covid.
Instead, they randomly assigned their trial participants to either a vaccination or a placebo. They then waited for participants with Covid symptoms before identifying the number in each group.
Vaccine efficacy is calculated using a standard methodology, which is based on the relative difference between the fraction of vaccinated participants that got Covid vs. the fraction of unvaccinated participants with Covid (shown below). Assuming Moderna assigned the placebo and vaccine evenly across 30,000 participants, the number does work out to 94.5%.

Back to the question of whether the chance of getting Covid symptoms after being vaccinated is 5.5% — well, I shall quote the New York Times:
A 95 percent efficacy is certainly compelling evidence that a vaccine works well. But that number doesn’t tell you what your chances are of becoming sick if you get vaccinated. And on its own, it also doesn’t say how well the vaccine will bring down Covid-19 across the United States. — New York Times (Nov 20)
This then brings us to our next pertinent question.
Question #2: Does the 95% effectiveness rate generalize to me, if I am a high-risk individual above the age of 65?
Well, here is where I am not comfortable with the lack of transparency.
Moderna, in keeping with the priority of saving the lives of high-risk individuals, did include a sizable number of individuals above 65 years.
The COVE study includes more than 7,000 Americans over the age of 65. — Moderna, Nov 16 press release
Subsequently, they report that “the 95 COVID-19 cases included 15 older adults (ages 65+)”, which is 15.8% of the total number of cases. However, what they did not disclose was the distribution of these older adults.
Given that we know that only 5 vaccinated people came down with Covid symptoms, there are two extremes in terms of possible scenarios:
- All 15 of these 65+ year olds were in the placebo group. In other words, zero cases in the vaccinated group — once vaccinated, any 65+ year old was protected from Covid symptoms, hurrah!
- All of the 5 that fell sick with Covid in the vaccinated group were 65+ year olds. In other words, the efficacy of the vaccine was not as high as 95% for this particular age group — in fact, it comes close to 50% (table below)

Well, it is my personal view that it is unlikely that the first scenario happened because if so, Moderna would have more reason to share this result. Rather, if any of the other 5 scenarios happened, their claim to a 95% efficacy becomes a little shakier, especially in the context of groups where it matters the most.
On this note, what about the 5,000+ Americans under the age of 65 but diagnosed as high-risk by Moderna. Why not mention their count alongside the breakdown of other groups across the 95 Covid cases?
It also includes more than 5,000 Americans who are under the age of 65 but have high-risk chronic diseases that put them at increased risk of severe COVID-19, such as diabetes, severe obesity and cardiac disease. — Moderna, Nov 16 press release
What appears to be selective disclosure of information does not inspire confidence in me as a layman. Thankfully, it appears from other sources that “the company plans to release additional results later, including effectiveness in specific groups such as the elderly.” (source) We will have to wait and see.
Question #3: With a 95% effectiveness, does this mean that Covid transmission will be halted in its tracks?
Notice that the first question referenced getting “sick with Covid” and not getting “infected with Covid”. In both vaccine trials, it appears that the Covid patients in the trials were identified based on their symptoms.
If volunteers developed symptoms like a fever or cough, they were then tested for the coronavirus. — New York Times, Nov 20
Hence, while preliminary trial data does show that the vaccines do reduce symptomatic infections, there remains a possibility that the vaccine did not prevent participants from getting asymptomatic infections at the same 95% efficacy.
‘When we start the deployment of this vaccine, we will not have sufficient concrete data to prove that this vaccine reduces transmission.’— Tal Zaks, Moderna Chief Scientist
As far as evidence shows, people who are asymptomatic can still spread the virus to others. In a cruel paradox where vaccinated people are still at risk of being asymptotically infected, they could engage in riskier activities that lead to them spreading Covid at a higher rate. This could be particularly deadly before a sizable part of the population has been vaccinated.
Which leads me to the most important and difficult question of them all:
Question #4: Once I get vaccinated, does this mean I can go out and live life as it was pre-Covid?
This is a tough question on so many fronts, with so many factors to consider. The considerations go beyond myself to the impact I may have on others, especially the high-risk populations. Perhaps it makes sense to start by thinking about what causes Covid deaths.
This is most probably a gross over-simplification but if I could identify three key factors driving the number of Covid deaths in the U.S., it would be:
- The level of transmission within the population,
- The level of human interaction within the population,
- The risk of dying from a Covid infection
The first two factors drive an individual’s likelihood of getting infected with Covid whereas the third determines the transition from a state of infection to death.
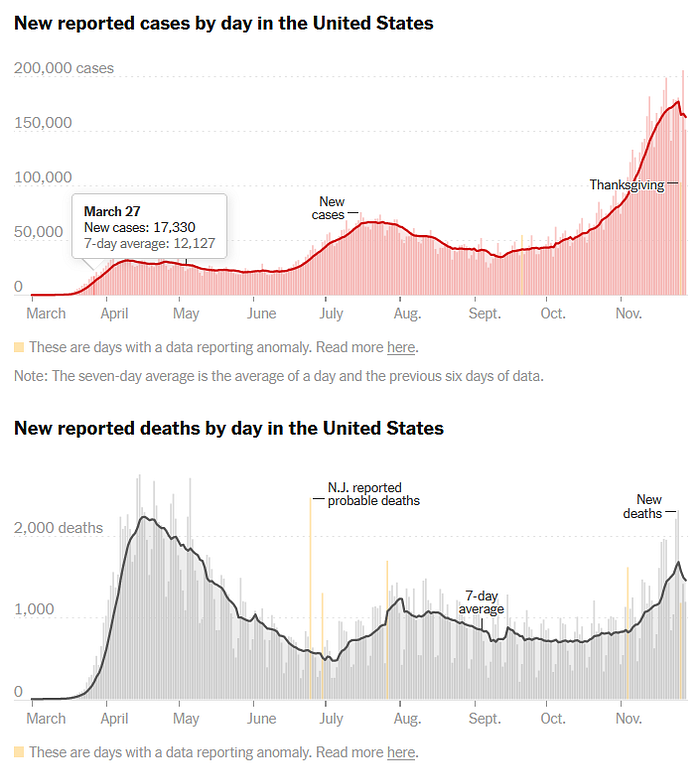
This also explains despite the number of U.S. daily positive cases going up in June, the number of deaths continued to decrease (graphs below). Besides the fact that healthcare providers were gaining experience with the virus, studies have shown that a younger, healthier group of people were getting infected and were arriving at hospitals with less severe symptoms than those infected in the spring. This is most probably a consequence of the elderly being relatively more cautious (by reducing their level of human interaction) but it shows how deaths can be prevented by reducing the average risk of a Covid victim dying from the virus.
This sounds like great news since getting a vaccination does seem like the equivalent of moving someone from a high-risk group to a lower-risk group — i.e. reducing their risk of dying from Covid.
Wait a second though — if we zoom out and look at the reported cases vs. deaths in the US since June, it is not a pretty sight. Deaths are slowly climbing back up once again, getting closer to the levels experienced in April — May.
Bringing this discussion back to the vaccine —my personal view is that while it may lower the average Covid patient’s risk of dying from the infection, it is not 100% and we do not know (at this point) its effect on limiting asymptomatic Covid transmission.
If we do decide to resume human interaction as per normal (think 500-people rave parties) and the Covid remains rampant within the population, there is a small chance of those vaccinated developing symptoms (let’s say 5%). With larger population base exposed to the virus, this could make up a significant number of people. My oversimplified Wordart diagram below:

Also, can I just point out that as of November 2020, we do not know how long vaccine-induced Covid immunity may last. I quote the CDC:
Regarding vaccination, we won’t know how long immunity lasts until we have a vaccine and more data on how well it works. — CDC FAQ on Covid-19 Vaccination
So to answer my question, my personal conclusion right now is that the return to pre-Covid life will most probably have to be done in a phased and careful fashion. I will have to be reminded not to get too complacent too quickly.
Beyond issues relating to the vaccine’s efficacy, there are further pieces of the puzzle which have to fall into place before a vaccine can be truly effective. Vaccine efficacy is “typically measured under optimal conditions where vaccine storage and delivery are monitored” (CDC). This could differ greatly from actual effectiveness under real-world conditions.
Evidence in the news also points to major challenges on the logistical front that have to be surmounted, given the cold storage challenges and the lack of public trust. Immunization experts have cautioned against a “build it and they will come” approach, which is valid considering that 42% of U.S. adults polled have said that they would not get a vaccine.
To distribute those vaccines, the US must undertake the most logistically difficult vaccination campaign in history, with a hesitant and weary public, and at least one vaccine with unprecedented storage requirements. — The Guardian
Finally, despite sounding like a wet blanket, I want to state for the record that I view the vaccines as a triumph of science. Yet, having done some desktop research of my own, my take is that the fight to save the world from Covid is far from over. For now, I’m keeping that safe 6-feet distance away from the roller-coaster of unbridled optimism.
“If I advocate cautious optimism it is not because I do not have faith in the future but because I do not want to encourage blind faith.” — Aung San Suu Kyi
